Introduction
More than 70% of patients with cancer, especially in the advanced stages, develop the signs and symptoms of cachexia and about 20% die from the consequences of this syndrome.
Cancer cachexia can be defined as a multifactorial syndrome characterized by progressive loss of muscle mass (with or without loss of lean mass), which cannot be completely corrected with conventional nutritional support and which leads to progressive functional damage.
The characterizing aspects of neoplastic cachexia are commonly weight loss (especially muscle mass) and inflammation. This leads to the main symptoms of the cachectic patient, such as anorexia, anemia, fatigue, which contribute to the complex clinical picture and to the impairment of the patient's quality of life.
Regardless of the patient's BMI category, a correlation has been demonstrated between the extent of weight loss, and in particular muscle mass loss, and survival.
The incidence of weight loss at the time of diagnosis varies significantly, depending on the location of the tumor.
The metabolic alterations that characterize cancer cachexia include:
Increased energy consumption
at rest
Loss of muscle mass, resulting from increased proteolysis and reduced protein synthesis
Loss of fat mass due to increased lipolysis, resulting from both specific mediators produced by the tumor and increased gluconeogenesis
Reduced intake of energy substrates with the diet, as a consequence of symptoms such as anorexia, nausea and vomiting
Difficult use of newly formed glucose for hypoinsulinemia and / or peripheral resistance to insulin
Oxidative stress, with consequent damage to DNA, membrane lipoproteins and central enzymes and coenzymes in regulating the main cellular metabolic pathways
Evaluation of neoplastic cachexia
Unintentional weight loss is the first diagnostic criterion for cancer cachexia.
According to a consensus paper, neoplastic cachexia should be suspected if there is:
- Unintentional weight loss of more than 5% of weight over 6 months or
- Weight loss of > 2% in a patient with a BMI <20 or with a diagnosis of sarcopenia.
The assessment of body weight and its changes over time is recommended in the cancer patient at the time of diagnosis and periodically during the course of the disease in order to make a timely diagnosis of neoplastic cachexia.
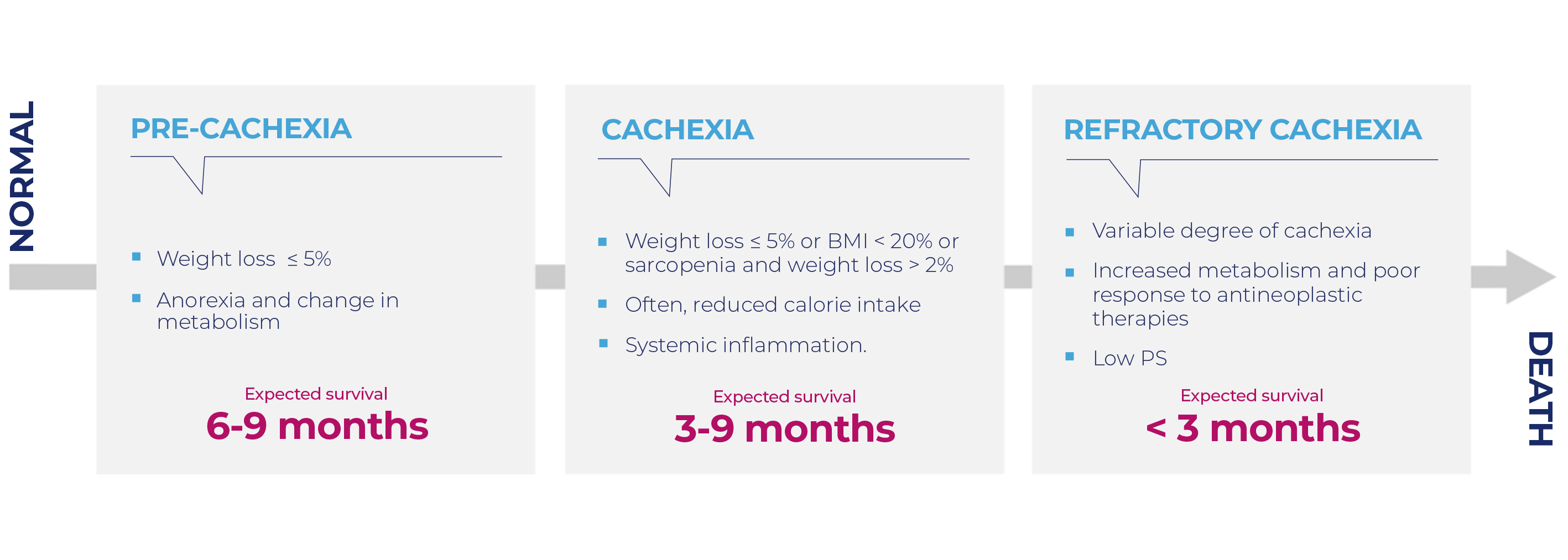
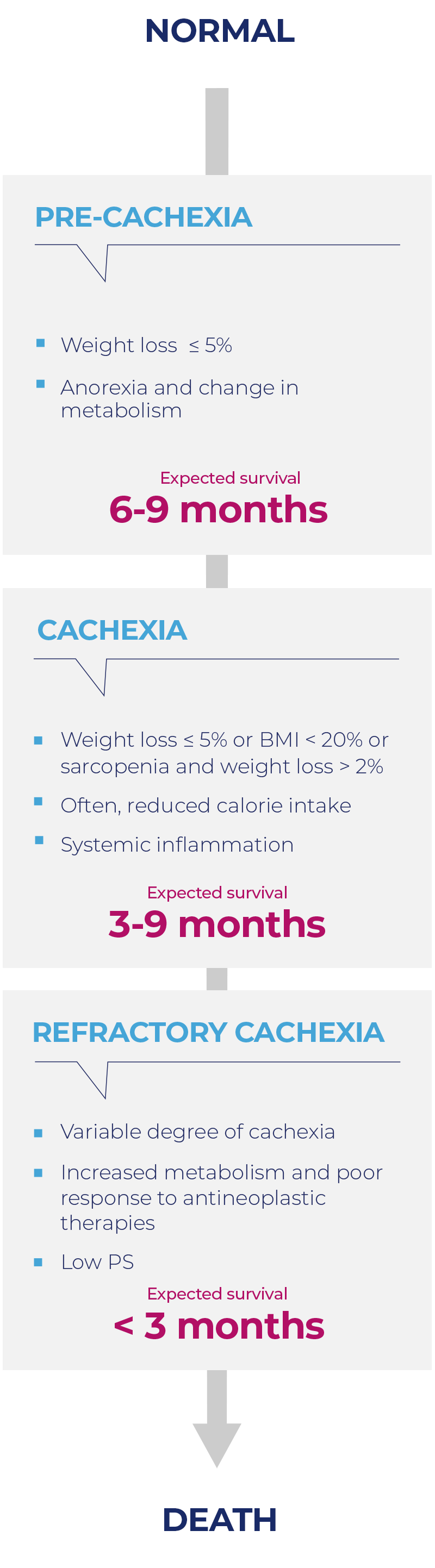
The diagnosis of cachexia must necessarily include other criteria besides pure weight loss, such as the presence of muscle loss, anorexia and inflammation. The evaluation of these parameters also allows classifying the degree of severity of cachexia. Indeed, neoplastic cachexia evolves through various stages: from pre-cachexia to full-blown cachexia up to refractory cachexia.
Treatment
The treatment of cachexia must take into account the patient's prognosis and the presence of uncontrolled symptoms (nausea, vomiting, constipation, pain, etc.). The type of approach and objectives vary according to the degree of severity of cachexia.
Pre-cachexia
Therapy options for late-stage cachexia remain poor. Therefore, it is essential to initiate treatment as early as possible.
Pre-cachexia therapy
is based on:
- Food counseling
- Control of concomitant symptoms
- Possible administration of nutritional supplements
- Possible administration of Megestrol acetate (MA)
Cachexia
Treatment should be aimed at regaining body weight and muscle mass or, in the alternative, avoiding further deterioration.
These objectives can be achieved with a multimodal approach, established on the basis of a thorough evaluation and periodic monitoring of the diagnostic parameters.
Cachexia therapy
is based on:
- Nutritional / dietary support
- Administration of MA / MPA
- Administration of anti-inflammatory drugs
- Treatment of concomitant symptoms
- Disease-oriented treatment, with the aim of reducing the hypercatabolism associated with the neoplasm
Refractory cachexia
The goal of treatment is not the recovery of weight loss, but the control of symptoms and the improvement of the patient's quality of life.
Patients with refractory cachexia have a shortened life expectancy, which does not allow effective anticachectic treatment.
At this stage, the cost and risks of artificial nutrition outweigh the benefits.
Therapy should be aimed at alleviating the consequences and complications of cachexia and controlling concomitant symptoms.
Nutritional support
All types of nutritional support can be used in cancer patients, from the prescription of an adequate diet, to the integration with specific oral products, to the enteral or parenteral nutrition in hospital or at home.
The choice depends on the patient's nutritional status, digestive tract function, therapeutic program and prognosis.
Pharmacological approach
Progestogens: megestrol acetate and medroxyprogesterone acetate are currently the only drugs with ministerial therapeutic indication for cachexia, not only of neoplastic origin.
The rationale for their use comes from both experimental and clinical studies. Progestogens induce a reduced synthesis and release of pro-inflammatory cytokines in treated patients, and this mechanism appears to be the main cause of the anti-cachectic effect.
The AIOM guidelines recommend, with a strong positive clinical recommendation, the use of progestogens in patients with cachexia since these drugs have been shown to induce an improvement in appetite and body weight, even though without modifying muscle mass.
Progestogens could also be used in patients with refractory cachexia and those in whom anorexia is the most relevant symptom.
Severe side effects are of rare incidence. The only side effect significantly more frequent than placebo was the edema of the lower limbs. Synthetic progestogen therapy is contraindicated only in case of diabetes, severe liver damage, hypercoagulability or severe hypertension.