Introduction
Many stimuli can cause nausea and vomiting, such as adverse drug reactions (most commonly chemotherapy drugs, thus inducing CINV - Chemotherapy-Induced Nausea and Vomiting), radiation exposure (as in radiation therapy for cancer, thus inducing RINV - Radiotherapy-Induced Nausea and Vomiting), infections, CNS disorders (such as seizures and migraines) and hormonal causes (such as pregnancy). Nausea and vomiting can also occur after surgery (PONV - Post-Operative Nausea and Vomiting).
Focus on: CINV
If left untreated, CINV can affect between 60% and 80% of cancer patients.
Preventing nausea and vomiting is the primary goal of all major oncology scientific societies (AIOM, ESMO, ASCO and NCCN). Therefore, antiemetic therapy should be started before the administration of chemo/radiotherapy and should be prescribed as early as the first cycle of treatment.
If nausea and vomiting can reduce a patient's quality of life and increase the cost of health care. Still, the biggest problem with issues such as CINV is that it can prevent patients from completing chemotherapy, resulting in up to 50% of patients delaying or refusing possible life-saving cancer therapy.
Risk factors predisposing to the occurrence of CINV
1. Patient characteristics
- Age: < 55 years
- Female
- Low or no alcohol consumption
- History of motion sickness
- Previous nausea and vomiting: women with a history of nausea and vomiting in pregnancy are more susceptible to emesis
- Anxiety
2. Types of chemotherapeutic agents
Chemotherapy agents, by their nature, tend to cause vomiting.
Every agent carries a risk of side effects, including vomiting, regardless of the type of patient receiving the treatment. Therefore, this is a problem involving many types of cancers.
For this reason, when starting chemotherapy and radiotherapy, it is important to start an antiemetic treatment as prophylaxis.
When receiving treatment using agents in the highest risk category, which includes cisplatin, higher-dose cyclophosphamide (≥1500 mg/m2), and many other agents, there is a greater than 90% chance that a patient will develop CINV if not receiving prophylactic antiemetics in parallel.
Treatment
Patients undergoing cancer chemotherapy present three different types of emesis, each of which requires a different prophylactic and therapeutic approach due to the varied characteristics:
- Acute emesis, which occurs within the first 24 hours after administration of the anticancer drug.
- Delayed emesis, which occurs starting more than 24 hours after the administration of chemotherapy and may persist for multiple days or even until the subsequent cycle of chemotherapy.
- Anticipatory emesis occurs immediately prior to the administration of cancer chemotherapy in patients with previous experience of acute or delayed emesis from chemotherapy. It is usually triggered by the sight and/or smell of the clinic where the therapy is administered.
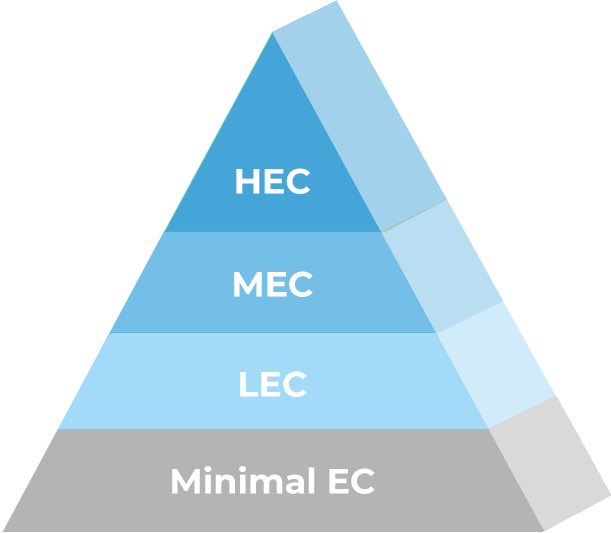
Emetogenic potential of anticancer drugs (4 groups)
The emetogenic potential of anticancer drugs, depending on whether they are administered parenterally or orally, is classified into four groups: high (risk of emesis > 90%), moderate (between 30 and 90%), low (between 10 and 30%) and minimal (< 10%). This classification is arbitrary because the emetogenic characteristics of many drugs (frequency, intensity, duration, onset time after administration, etc.) are not known.
In addition, the emesis induced by an anticancer drug also varies according to its possible combination with other anticancer drugs, to the dose, to the duration of infusion and to some patient characteristics such as sex, age, previous experience of emesis during pregnancy, kinetosis, etc.
1. Highly emetogenic chemotherapy (HEC): risk of emesis 90%
2. Moderately emetogenic chemotherapy (MEC): risk of emesis between 30% and 90%
3. Low emetogenic chemotherapy (LEC): risk of emesis between 10% and 30%
4. Chemotherapy with Minimal emetogenic power: risk of emesis between <10%
Anti-emetics
Pharmacological Classes
Classes of antiemetics with a high therapeutic index
| Classes | Active ingredient |
|---|---|
| Antagonists of 5-HT3 receptors | Ondansetron Granisetron Palonosetron |
| Receptor antagonists 1 antagonists of neurokine (antagonists of P substance receptors) |
Aprepitant Fosaprepitant Netupitant |
| Corticosteroids | Desametasone Metilprednisolone |